Imaging the acute abdomen
Jennifer O. Brisson, DVM, DACVR
Massachusetts Veterinary Referral Hospital, Woburn, MA
Posted on 2017-06-27 in Diagnostic Imaging and Emergency & critical care
The acute abdomen is a common presentation in emergency veterinary medicine. The term acute abdomen refers to a patient presenting with acute clinical signs and abdominal pain due to a disease process of an abdominal structure. In veterinary medicine, this commonly includes gastrointestinal, hepatobiliary, or urogenital causes, as well as those occurring secondary to abdominal neoplasia. Gastrointestinal emergencies include dietary indiscretion mechanical ileus (foreign material obstruction), intussusception, gastric dilatation and volvulus, and pancreatitis. Urogenital causes include urethral obstruction, ureteral obstruction, and pyometra. Obstruction of the biliary tract, either at the level of the gallbladder such as mucocele formation, or the ducts, are also possible diagnoses for the acute abdomen. Many of the these may lead to septic peritonitis if there is rupture or perforation of the affected structure. Some forms of neoplasia, such as splenic hemangiosarcoma, cause acute hemorrhagic effusion and cardiovascular collapse.
Trauma is another potential cause of acute abdomen signs. Patients that have been stuck by a motor vehicle or been involved in an altercation with another animal (wildlife and domestic) can have multiple injuries concurrently contributing to their signs. Initial radiographs and ultrasound can be very informative but many of these patients require whole body CT examination to determine to full extent of their injuries. CT examinations are also extremely informative for surgical planning.
Determination of the underlying cause for an acute abdomen begins with the patient history, signalment and physical exam findings. These are essential for assessment. Diagnostics including radiography, ultrasonography, and cytology are often used. In advanced care settings, computed tomography (CT) may also be performed.
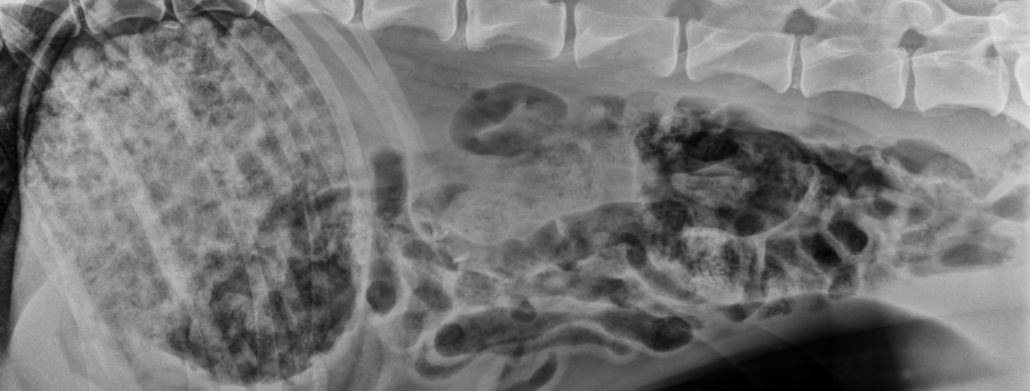
Abdominal Radiography
A standard series of abdominal radiographs includes a right lateral (RL) and ventrodorsal (VD) projection. For cases presenting with clinical signs of acute abdomen a three-view series is recommended, with the additional view of the patient in left lateral recumbency (LL). The LL view is informative to the position and contents of the pylorus, pyloric-duodenal junction and duodenum. Additional views can increase sensitivity to the detection of abdominal pathology, for example, identification of free peritoneal gas when septic peritonitis is suspected. A dorsoventral (DV) view of the abdomen is of limited usefulness, and should be employed on a limited basis, for example to assess gastric position.
Abdominal ultrasonography
Ultrasound is an essential tool for assessment of the acute abdomen patient. Point of care assessment techniques such as Focused Assessment with Sonography for Trauma (FAST) are routinely employed in a variety of medical settings, including general practice and emergency specialty care veterinary hospitals. FAST ultrasound exams were initially developed for use in the human emergency room setting as a point of case assessment tool, and evolved to be used for monitoring as well. The use of FAST exams have been investigated in veterinary medicine, and are now well documented in the veterinary literature (Boysen, 2004; Lisciandro 2009). FAST exams have been further developed to specifically assess the abdomen (AFAST), thorax (TFAST), and lungs (Vet BLUE), among others (Lisciandro 2011; Lisciandro 2014).
AFAST exams, as the name implies, are focused on the abdomen and can demonstrate abdominal effusion, peritonitis, urinary bladder rupture and numerous other pathologies. AFAST can detect small volumes of free abdominal fluid comparably to CT, considered the gold standard, and with greater sensitivity than physical examination or radiography. As such, AFAST exams are an invaluable tool for the evaluation of an acute abdomen patient.
To perform an AFAST exam, the patient is placed in RL recumbency or if unable to accommodate that positioning, a modified sternal recumbency. Four standard views (or acoustic windows) are recommended to assess the abdomen.
- Diaphragmatic-hepatic (DH) view: probe placed under/caudal to xiphoid process to visualize cranial abdomen including diaphragm, liver, gallbladder, and biliary tract. Can also visualize caudal pleural and pericardial spaces in most patients.
- Spleno-renal (SR) view: probe placed along left lateral body wall caudal to 13th rib to visualize spleen, left kidney, pancreas, peritoneal and retroperitoneal spaces.
- Cysto-colic (CC) view: probe placed in caudal abdomen along ventral midline to visualize the urinary bladder, uterus, intestine, colon, and caudal abdominal recesses.
- Hepato-renal (HR) view: probe placed ventral to the umbilicus to visualize intestine, peritoneal space, right kidney, right liver, +/- spleen.
Repetitive sequential evaluation across patients will increase knowledge and familiarity with anatomy and disease pattern recognition, increasing the overall sensitivity of the ASFAT exam with an experienced user.
AFAST may be used alone in the evaluation of an acute abdomen patient, or in conjunction with a complete diagnostic abdominal ultrasound examination. During a complete diagnostic abdominal ultrasound examination, the patient is placed in dorsal recumbency and sequential evaluation in both the longitudinal and transverse planes is performed of the liver, spleen, kidneys, adrenal glands, urinary bladder, gastrointestinal tract, lymph nodes, mesentery, vasculature, and reproductive structures. This type of ultrasound exam is more typically performed by an experienced specialist, such as a board-certified radiologist or internist. Detection of pathology and extent of disease can often be garnished from these exams, and lead treatment plans to include fluid sampling, tissue sampling, endoscopy, and surgical intervention.
Abdominal Computed Tomography (CT)
Abdominal CT examinations may be performed for patients that ultrasound or radiography alone does not provided enough information, is unavailable, or size of patients creates limitations (giant breed dogs). Causes of acute abdomen that may need CT for further evaluation include severe peritonitis (Ex. septic peritonitis secondary to teriyaki stick ingestion and migration), mesenteric or colonic torsion, trauma, and neoplasia. With the advancement of multidetector CT technology and availability in veterinary medicine, many CT exams may now be performed with mild sedation and no longer require general anesthesia.
The role of diagnostic imaging in patients with acute abdomen is not limited to use as a diagnostic tool, but can also be used to facilitate surgical planning, interventions, treatments, and response thereto.
Further reading
- Boysen SR, Rozanski EA, Tidwell AS, et all. 2004. Evaluation of a focused assessment with sonography for trauma protocol to detect free abdominal fluids in dogs involved in motor vehicle accidents. J Am Vet Med Assoc 225(8):1198-1204.
- Lisciandro GR, ed. 2014. Focused Ultrasound Techniques for the Small Animal Practitioner. Ames, Iowa. Wiley Blackwell.
- Lisciandro GR, Lagutichik MS, Mann KA, et all. 2009. Evaluation of an abdominal fluid scoring system determined using abdominal focused assessment with sonography for trauma in 101 dogs with motor vehicle trauma. J Vet Emerg Crit Care 19(5):426-437.
- Lisciandro GR. 2011. Abdominal and thoracic focused assessment with sonography for trauma, triage, and monitoring in small animals. J Vet Emerg Crit Care 21(2):104-122.
- Lisciandro GR, Fosgate GT, Fulton RM. 2014. Frequency and number of ultrasound lung rockets (B-lines) using a regionally based lung ultrasound examination named vet BLUE (veterinary bedside lung ultrasound exam) in dogs with radiographically normal lung findings. Vet Rad Ultrasound 55(3):315-22.
About the author
|
 Dr. Brisson received her Doctor of Veterinary Medicine with thesis, from Tufts University, Cummings School of Veterinary Medicine in 2004. She completed a one year internship in small animal medicine and surgery at the Veterinary Referral and Emergency Center in Norwalk, CT, followed by a three year residency in Diagnostic Imaging at Tufts University in July of 2008. Dr. Brisson became board certified by the American College of Veterinary Radiology in September 2009. Dr. Brisson has received extensive training in all modalities of veterinary radiology, including magnetic resonance imaging (MRI), computed tomography (CT), radiography, nuclear medicine, and ultrasound. Her professional interests in diagnostic radiology include abdominal MRI, gastrointestinal and hepatobiliary ultrasound, and thoracic computed tomography. Dr. Brisson also has a strong professional interest in Interventional Radiology. Dr. Brisson joined the radiology department at Massachusetts Veterinary Referral Hospital in July 2009. In 2014 she was promoted to Assistant Medical Director for the surgical services.
Dr. Brisson received her Doctor of Veterinary Medicine with thesis, from Tufts University, Cummings School of Veterinary Medicine in 2004. She completed a one year internship in small animal medicine and surgery at the Veterinary Referral and Emergency Center in Norwalk, CT, followed by a three year residency in Diagnostic Imaging at Tufts University in July of 2008. Dr. Brisson became board certified by the American College of Veterinary Radiology in September 2009. Dr. Brisson has received extensive training in all modalities of veterinary radiology, including magnetic resonance imaging (MRI), computed tomography (CT), radiography, nuclear medicine, and ultrasound. Her professional interests in diagnostic radiology include abdominal MRI, gastrointestinal and hepatobiliary ultrasound, and thoracic computed tomography. Dr. Brisson also has a strong professional interest in Interventional Radiology. Dr. Brisson joined the radiology department at Massachusetts Veterinary Referral Hospital in July 2009. In 2014 she was promoted to Assistant Medical Director for the surgical services.

