The shocking truth about non-cardiogenic pulmonary edema
Patty Pate, CVT, VTS(ECC), CCFE
Port City Veterinary Referral Hospital, Portsmouth, NH
Posted on July 26, 2016
Non-cardiogenic pulmonary edema (NCPE) is defined as a pathologic accumulation of fluid within the lungs of a patient without primary cardiac disease. It results from an increase in permeability at the alveolar-capillary bed coupled with an increased hydrostatic pressure in the vasculature surrounding the lungs. A number of conditions can cause NCPE and therefore it can be routinely seen in the clinical setting. Knowing how it happens, what to expect, and how it is treated can help enhance the care of the patient.
Etiology/Pathophysiology
In order to understand non-cardiogenic pulmonary edema, one needs to know how it differs from cardiogenic pulmonary edema (CPE). A patient suffering from cardiogenic pulmonary edema has a primary problem with its heart, which in turn reduces stroke volume. Decreased cardiac output leads to poor filtration by the kidneys leading to fluid accumulation within the vasculature. When the patient’s heart condition affects the left side of the heart, hydrostatic pressure backs up into the capillary beds surrounding the lungs. As intravascular volume overpowers the stretch capacity of these capillary beds, a transudate effusion leaks out of the vasculature and into the alveoli they encompass.
Non-cardiogenic pulmonary edema can be broken down into three types: neurogenic, post-obstructive and ARDS/ALI. All three have a slightly different etiology and pathophysiology but all three create an accumulation of protein-rich, exudate effusion in the lungs, resulting in respiratory distress.
Neurogenic pulmonary edema can occur secondary to conditions such as status epilepticus, head trauma, and electrocution and results from hydrostatic and pulmonary permeability changes. The inciting event creates a massive catecholamine release, leading to systemic vasoconstriction. This vasoconstriction creates an acute increase in hydrostatic pressure and severe hypertension in normovolemic patients. These changes are so acute that the alveolar epithelium and tight junction cells sustain significant damage and ultimately vascular leakage occurs.
Post-obstructive pulmonary edema can result after a patient has sustained any upper airway obstruction. Conditions such as laryngeal paralysis, strangulation, or foreign body occlusion have all been known to cause NCPE. The upper airway obstruction causes in acute increase in the patient’s thoracic negative pressure. This leads to a decrease in venous blood flow to the heart and an increase in pulmonary intravascular volume as blood pools. As the patient struggles to breath, the mechanical ventilatory stress creates pulmonary epithelial and endothelial damage. Hypoxia worsens leading to a sympathetic capillary vasoconstriction. The increase in pulmonary intravascular volume coupled with the capillary vasoconstriction leads to an acute increase in hydrostatic pressure. Since the pulmonary tissues have sustained damage, vascular leakage ensues.
Acute respiratory distress syndrome (ARDS) and acute lung injury (ALI) are true critical care syndromes that arise secondary to a local or systemic insult. It is a sequela to conditions that cause a profound systemic inflammatory response and results in pulmonary epithelial and endothelial damage and a subsequent increase in vascular permeability. The clinical symptoms of ARDS/ALI usually take anywhere from one to four days after the original insult. Patients with a primary pulmonary disease, such as pneumonia, or patients with a profound systemic disease, such as sepsis, are at increase risk for developing ARDS or ALI.
Clinical Presentation
Patients typically develop respiratory distress within one hour of the inciting event for both neurogenic and post-obstructive NCPE. They present with an increased respiratory rate and effort, sometimes accompanied by orthopnea.
First, the patient needs to be assessed for any ongoing airway obstruction. If one is appreciated, immediate emergency interventions need to be taken to regain a patent airway.
Next, a thorough history and assessment of the patient’s cardiovascular system are important to rule out cardiogenic pulmonary edema. Cardiac auscultation, palpation of pulse quality and capillary refill time (CRT) measurement can help to rule out primary cardiac disease. Patients with primary cardiac disease may be found to have arrhythmias, murmurs, weak/thready pulses, and prolonged CRT’s.
Stabilization
Patients clinical for their NCPE need to receive oxygen supplementation as soon as possible. As with any patient in respiratory distress, treatments need to be done in a methodical step-by-step fashion because they have little tolerance for any added stressors. The focus of stabilization should be limited to oxygen supplementation to help alleviate the patient’s hypoxemia and intravenous catheter placement for quick venous access should the patient progress to cardio-pulmonary arrest. In the event of electrocution, pain management should be seriously considered as pain can exacerbate the patient’s mechanical ventilatory efforts.
Diagnostic Findings
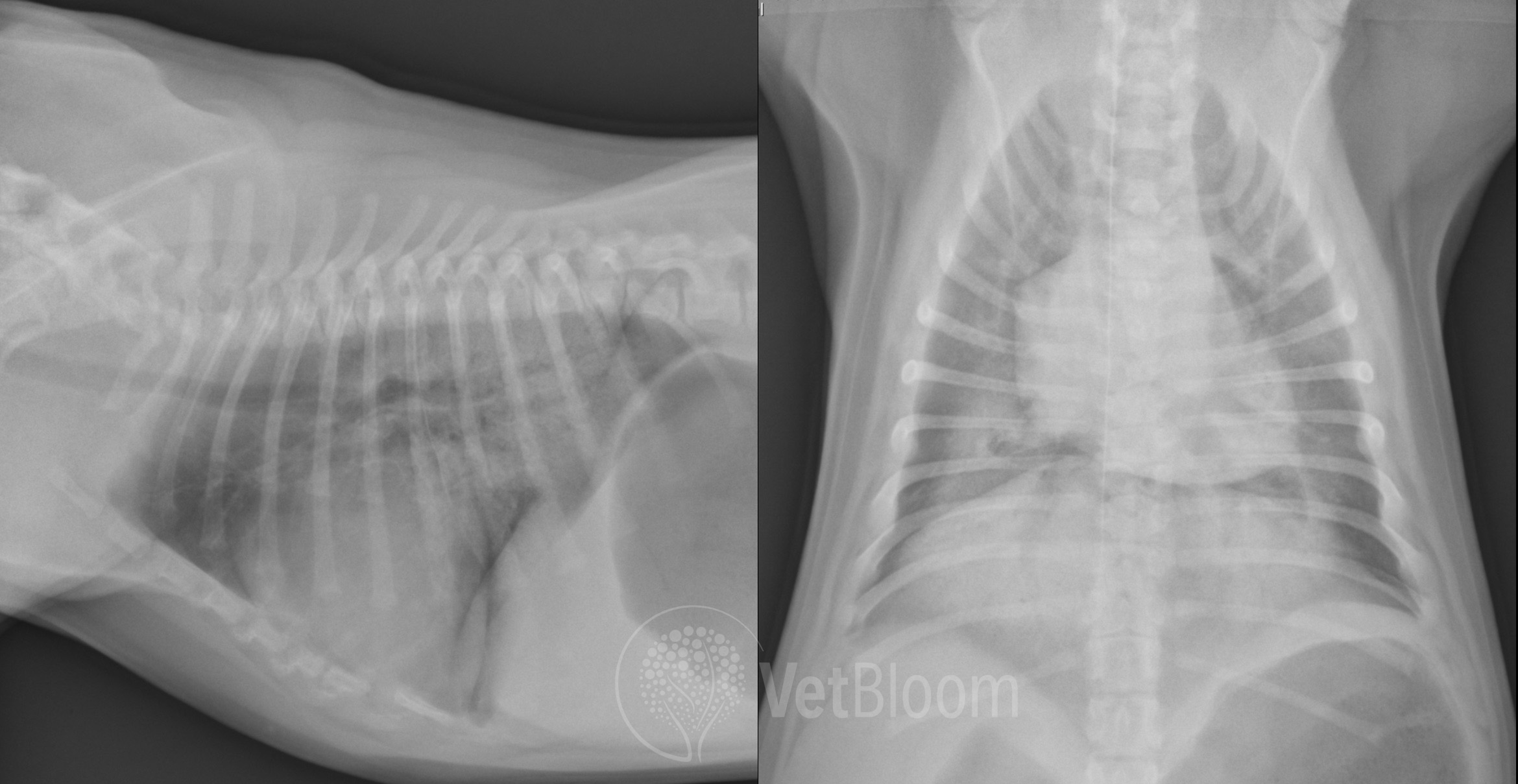
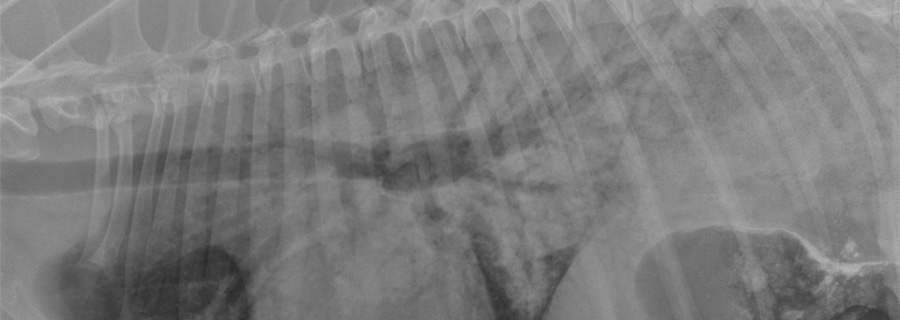
Fig. 1: Non-cardiogenic pulmonaryedema in a dog that experienced a near drowning.
Three-view thoracic radiographs (fig. 1) are needed to diagnose NCPE. These images help to determine the severity of pathology. NCPE has a hallmark pulmonary infiltrative pattern within the caudodorsal lung fields. In cases with ARDS/ALI, all lung fields may be affected.
An arterial blood gas sample can be obtained to further determine the patient’s status. Information such as acid/base abnormalities and ventilation/perfusion abilities can be assessed. Ideally, in order to obtain baseline values, this sample should be drawn from a patient breathing room air for 10-15 minutes prior to sampling. Arterial blood sampling is invasive and requires a high degree of skill to be performed quickly. It is not always possible depending on the severity of the patient’s dyspnea but if the patient tolerates the venipuncture, it is an ideal method for determining ventilatory status. Any patient with a partial pressure of dissolved oxygen (PaO2) less than 80 mmHg while breathing room air is considered hypoxemic and supplemental oxygen should be considered. Further information can be obtained by calculating an Alveolar-arterial gradient (A-a gradient). The A-a gradient is the comparison of oxygen concentrations in the alveoli to that of arterial blood. Values >20 can be indicative of a ventilation/perfusion mismatch.
Pulse oxymetry can be utilized to assess a patient’s oxygen hemoglobin concentration (SpO2) if the patient is not tolerant of arterial sampling. Pulse oxymetry is quick, non-invasive and easily tolerated by most patients. Normal SpO2 values of a patient breathing room air are 95-99%. Patients with an SpO2 of <93% are considered hypoxemic and require oxygen supplementation.
Additional blood work including a complete blood count, chemistry profile, urinalysis and coagulation tests should be obtained in order to identify any systemic abnormalities that may be contributing to the patient’s NCPE.
Treatment/Nursing Considerations
Non-cardiogenic pulmonary edema is usually self-limiting and clinical symptoms can resolve in as early as 18-24 hours after onset. The focus of treatment is typically supportive in nature with oxygen therapy and time being treatment staples. Fluid therapy and pharmacological-agent administration can be considered on a case-by-case basis.
Oxygen supplementation should be initiated at 40-70% fraction of inspired oxygen (FiO2). Oxygen chambers and nasal oxygen cannulas are ideal methods for continuous supplementation. The goal of therapy should be for the patient to easily maintain a PaO2 above 80 mmHg or an SpO2 ≥ 95%. If a PaO2 ≥ 60mmHg cannot be obtained with oxygen supplementation, continuous ventilation is warranted.
Fluid therapy can be beneficial to patients being treated for NCPE. Many do not feel well enough initially to eat or drink on their own. Isotonic crystalloids can be administered to maintain proper hydration and replace sensible and insensible losses. Fluid therapy, however, is not without risk in patients with NCPE. An increase in intravascular volume can lead to increased pulmonary hydrostatic pressures so fluid rates should be kept conservative. Colloid therapy may need to be considered in patients who are not hemodynamically stable. Hetastarch® and Vetstarch® are large molecular hydroxyethyl starches that help to maintain colloidal oncotic pressure and support blood pressure. These solutions should be avoided in any patient where severe pulmonary endothelial damage is suspected as these large molecules will leach into the alveolar spaces. This will cause free water to follow and exacerbate the patient’s condition.
Very few medications help to resolve NPCE. Some debate has been had over whether or not furosemide can be therapeutic in treatment of NCPE. Furosemide is a loop diuretic used to promote free water and salt excretion by the kidneys and is extremely effective in the treatment of cardiogenic pulmonary edema. The mechanism of action found to help CPE is not beneficial for patients with NCPE due to their epithelial disruption and exudative effusion. Some studies have found that a low dose constant rate infusion of furosemide can be beneficial to patients with NCPE in other ways by decreasing the pulmonary capillary pressures and reducing the amount of fluid “flooding” pulmonary tissues in patients with permeability changes. Furosemide has also been found to act as a bronchodilator and therefore can provide patient relief by reducing bronchospasms associated with NCPE.
β2 adrenergic agonists such as terbutilline and albuterol may also be used to help treat patients with NCPE. Although the efficacy of these drugs is unknown, it is believed that by triggering the receptors lining the alveolar epithelium, it can increase pulmonary fluid clearance. β2 adrenergic agonists can also provide some relief to the patient by reducing bronchospasms caused by NCPE. β2 adrenergic agonists should be used with caution as they have cardiogenic effects as well: increasing heart rate and blood pressure. These effects can increase pulmonary hydrostatic pressure, in turn exacerbating the patient’s NCPE. More research needs to be done to determine the true benefits, and these agents should be used as a last resort.
Nutritional support should be considered early in a patient’s treatment of NCPE, especially if the patient is suffering from oral burn lesions secondary to electrocution. These patients most likely will be reluctant to eat due to the level of dyspnea and/or discomfort. Placing a nasoesophageal or nasogastric feeding tube can be done quickly and with little stress. Patients may be fed liquid diets through these tubes to provide the essential nutritional management needed for these patients to heal quicker.
References
- Adamantos, S. & Hughes, D. Pulmonary Edema. In: Silverstein, D.C. & Hopper, K. (Eds.), Small Animal Critical Care Medicine. Louis, MO.; 2015: 116-119.
- Bachmann, M. & Waldrop, J.E. Noncardiogenic Pulmonary Edema. Compendium: Continuing Education for Veterinarians. 2012 Nov;34(11):E1
- Boothe, D.M. Drugs affecting the respiratory system. In: King, L.G. (Ed.), Textbook of Respiratory Disease in Dogs and Cats. Louis, MO: Elsevier; 2004: 487-497.
- Hawkins, E.K. Disorders of the Pulmonary Parenchyma and Vasculature. In: Nelson, R.W. & Couto, C.G. (Eds.) Small Animal Internal Medicine. St. Louis, MO: Mosby Inc.; 2009: 319-321.
- Hughs, D. Pulmonary Edema. In: King, L.G., (Ed.) Textbook of Respiratory Disease in Dogs and Cats. Louis, MO: Elsevier; 2004: 487-497.
- Presley, R.H. Noncardiogenic Pulmonary Edema. Veterianry Technician. 2006 June; 27 (6).
About the author
|