Tarsal osteochondrosis
Robert B. Hillman, DVM, MS, DACVS
Port City Veterinary Referral Hospital
The most common causes of pelvic limb lameness in adult dogs are cruciate disease and hip dysplasia. But when puppies present with lameness, we must avoid tunnel vision. Our differential list should be prioritized based on signalment. The following is a brief discussion of tarsal osteochondrosis including etiology and pathogenesis, clinical signs, diagnostics, treatment and prognosis. It is a combination of literature review and editorial based on clinical impression.
Etiology and pathogenesis
Osteochondrosis (OC) is a developmental orthopedic disease commonly observed in rapidly growing, large- and giant-breed, dogs, typically between five and ten months of age. Normally, the process of endochondral ossification involves physiologic calcification of the cartilage at the osteochondral junction and replacement by bone. When this fails to occur, a thickened focal area of degenerative cartilage results, outgrowing its nutrient supply. This area of necrotic cartilage is vulnerable to shearing forces encountered during normal weight bearing. This lesion is referred to as osteochondritis dissecans (OCD) when fissures are formed and joint fluid dissects (the dissecans part of OCD) between the cartilage and underlying bone, forming a flap. Cartilage degradation products reach the synovial fluid when a flap forms, causing synovitis, effusion, joint pain, and lameness. The cartilage flap may remain in situ and potentially reattach to subchondral bone or may dislodge forming a joint mouse. Joint mice may be resorbed in synovial recesses or remain in the joint, causing synovitis and osteoarthritis. The cause of OC has not been determined, but a combination of factors, including genetics, rapid growth, over nutrition and excess dietary calcium, trauma, ischemia, and hormonal influences, has been implicated.
The typical patients are puppies from predisposed breeds – typically large compared to littermates, having rapid growth rates, and are often on high planes of nutrition. The disease is most common in dogs that reach an adult weight of greater than 20 kg and tends to occur during periods of rapid growth. Puppies from small breeds of dogs are rarely affected with OC. After the shoulder and elbow, the tarsal joint is the third most common site of OC in the dog. While male dogs are more commonly affected than female dogs with OC in other sites, this sex difference has not been seen with tarsal OC. All of the patients treated for tarsal OCD at Port City in the last two years were young female Labradors. Like OC in other sites, it is usually noted between six to twelve months of age. Lesions are bilateral 40 % of the time. Right and left limbs are equally affected. The medial trochlear ridge is affected in 79 % of tarsal OCD cases, and 21 % involve the lateral ridge.
Breeds at risk for OC of the tarsus are the Bullmastiff, Labrador Retriever and Rottweiler. Bullmastiffs are 86 times more likely (odds ratio) to have tarsal OC than mixed breed dogs. The true odds ratio is 95% likely to be between 36 and 206 times (95% confidence interval). Rottweilers and Labrador retrievers account for 70 % of hock OCD cases.
Lesions may affect one or both trochlear ridges at multiple sites. The most common location is the plantar aspect of the medial trochlear ridge (80 % of cases). Seventy percent of cases affecting the lateral trochlear ridge involve the dorsal aspect. Rottweilers in one study accounted for 80 % of cases of lateral ridge OCD and 63 % of those cases had bilateral lesions.
Clinical signs
It has been reported that half the dogs presenting with tarsal OCD have a non-weight bearing lameness, although this has not been my personal experience. I mostly see pups with an intermittent but persistent moderate pelvic limb lameness. Perhaps the primary care vets in my area are more astute than most, and refer the cases before they become non-weight bearing. Lameness for those cases bearing weight usually worsens with exercise. There is typically palpable if not readily visible joint effusion. The affected joints usually have a decreased range of motion in flexion and may appear hyperextended.
Diagnosis
A presumptive diagnosis is made based on signalment and clinical signs. Tarsal OCD can be a difficult radiographic diagnosis. OCD of the medial trochlear ridge can be diagnosed on extended plain craniocaudal and slightly flexed mediolateral radiographs. Findings suggestive of medial OCD include increased joint space at the OCD defect, joint effusion and presence of an osteochondral fragment. A “sky-line” view of the tarsus with the joint flexed to 90 degrees and the x-ray beam directed perpendicular to the long axis of the tibia is often required to visualize OCD of the lateral trochlear ridge.
Radiographic evaluation should include standard lateral, flexed lateral, and dorsoplantar views of both tarsi. Additional views are also helpful, including a craniocaudal view of the proximal trochlear ridges, a dorsolateral-plantomedial oblique view (D45 L-PLMO), and a dorsomedial-plantolateral oblique view (D45 M-PLLO). The dorsal 45 degrees lateral-plantaromedial oblique (D45 degrees L-PMO) projection was the most useful in identifying the lateral lesions.
By the time you have taken six views of each tarsus, you might as well have done a CT – yes, even when comparing costs. One study compared a six-view study of each tarsus to CT and arthroscopic findings. Although the survey radiographs were sufficient to make a diagnosis, the CT examination helped to determine the exact site, and the number and size of the fragments of bone.
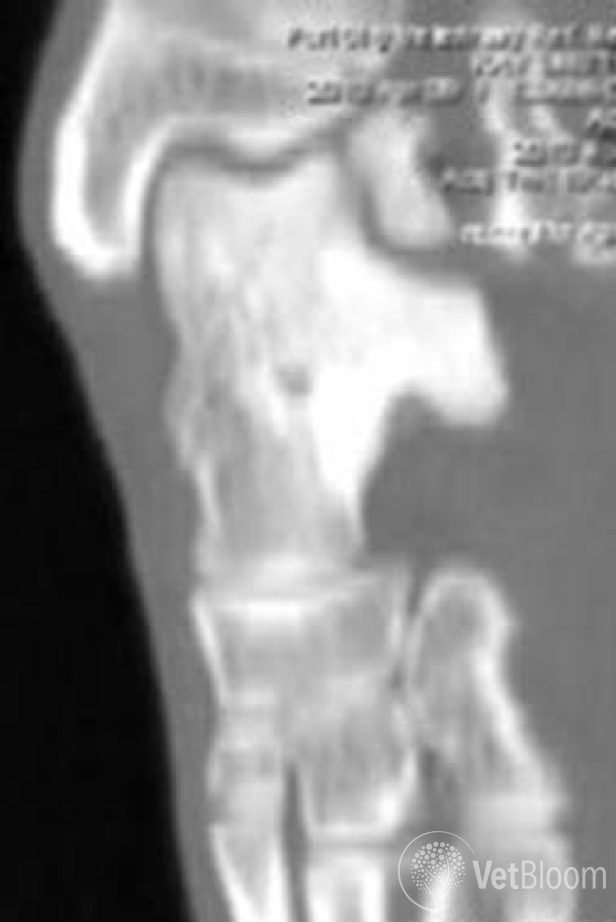
Fig. 1: CT image of lateral talar OCD lesion.
A CT scan is extremely helpful, because 40% of cases have bilateral lesions, lateral lesions can be difficult to identify and localize with radiography alone, and because the three dimensional image is invaluable in planning the surgical approach.
One retrospective study compared the value of radiographic CT imaging for the diagnosis of lateral trochlear ridge talar OCD. The flexed dorsoplantar sky-line and the plantarolateral-dorsomedial projections were the most reliable for radiographic detection of OCD fragments. While radiography detected OCD fragments in 8 of 11 joints, OCD fragments could be visualized and exactly localized by CT in all 11 joints. The ability to evaluate the talar ridges without superimposition of any bony structures is key.
Clearly CT is superior to radiography for localizing OCD fragments, especially on the lateral talar ridge. There are certainly many cases, particularly those involving the medial ridge, for which radiography would suffice for localization. I perform a CT on all tarsal OCD cases because of advantages in sensitivity and specificity and lesion localization. It helps me chose the least invasive approach to the lesion. Figure 1 is a CT reconstruction image of a seven-month-old female spayed Labrador with a large lateral talar OCD lesion. In this case, the fragment was too large to remove. A lateral approach using a fibular osteotomy, sparing the lateral collateral ligament, was used. The fragment was stabilized with a screw and wires. The osteotomy was stabilized with two screws (Fig. 2).
If you have a six month old Labrador, lame with a swollen hock that has decreased flexion, a set of radiographs prior to referral can be helpful, but is not essential. I am always going discuss the option of a CT with your clients. The CT is performed immediately pre-op, so there is only one sedation/anesthesia episode.

Fig. 2: Lateral (left) and AP (right) post-op radiographs of the dog described in the text and shown above in Fig. 1.
Treatment
Removal of the flap via small arthrotomy or arthroscopy and curettage of the bed is recommended. Some studies report about 1/3 of tarsal OCD lesions can be managed via arthroscopy alone. The rest require at least a mini-arthrotomy. As previously mentioned, CT is extremely helpful in planning the approach (medial or lateral, dorsal or plantar? Will maximal flexion or extension aid visualization? Will an osteotomy be required?). Dogs with lameness and a large flap appear to do better if operated early prior to the onset of DJD. Dogs with small lesions appear to have a better long-term prognosis. It has also been demonstrated that in dogs with bilateral tarsal OCD lesions found on CT but unilateral lameness, the nonclinical lesions were significantly smaller. Similar lesion size/prognosis correlations have been made with regard to OCD in the canine shoulder. Loss of a big piece of the trochlear ridge due to a large OCD defect or removal of excess bone (curettage) at surgery may cause increased joint instability and a poor prognosis.
In one study, sixteen joints with OCD treated with arthroscopy resulted in 10/14 dogs with lameness after exercise only, progression of DJD in most cases, and chronic lameness when comparing operated to unoperated limbs with force plate evaluation at a mean follow-up of 35 months.
Medical management for tarsal OCD is recommended in older dogs with severe regenerative changes. Most recent reports suggest that surgical intervention is preferred for treating tarsal OC. One study found no significant difference in long-term outcome between joints treated medically and those treated surgically, but that data is from nearly 30 years ago. Use caution if basing clinical decisions on old texts, and review articles citing review articles. The lack of difference in surgically and medically managed cases is more likely to be true in older dogs with chronic and significant OA. Surgical exploration and removal of the cartilage flap or osteochondral fragment can allow in-growth of fibrocartilage from the underlying subchondral bone. Early intervention with a minimally invasive approach is preferred. Once the lesion is exposed, the cartilage flap or osteochondral fragment is excised. Overall function is better with minimal curettage. There are some fragments that are simply too large to remove (i.e, the resultant defect would lead to joint instability). Large fragments can be stabilized with screw or wire fixation.
Prognosis
Time to maximal postoperative performance was 30 days or less in one study. Most cases have some gait abnormalities postoperatively, but are usually better than they were preoperatively. Dogs with OCD of the medial trochlear ridge seem to have more postoperative lameness than dogs with lateral trochlear OCD. Lateral OCD has less affect on the weight-bearing surface than medial OCD. Medical management may be needed long-term for treatment of DJD/OA.
The prognosis for OC of the tarsus after conservative therapy is guarded. Most dogs have intermittent lameness and moderate progression of OA. Even after surgery, OA is likely and often requires medical therapy to control pain and lameness. Despite the progression of OA noted radiographically after surgery, many dogs are clinically improved. Nevertheless, the prognosis remains guarded, because joint pain and lameness may recur as the OA progresses. One report sites faster recovery in dogs with lesions involving the non–weight bearing dorsal aspect of the lateral trochlear ridge. Several factors may influence the success of medical and surgical treatment, including the age of the dog, presence of OA, size of the osteochondral defect, presence of joint instability, site of the lesion, and whether the lesions are unilateral or bilateral.
Even though my tarsal OCD caseload has been fairly uniform in terms of signalment, I am surprised by the diversity of lesions found. After the thorough orthopedic exam, the consult involves discussing all options with the clients. Ensuring they understand the variable prognosis and different treatment options is important. While there may be occasional cases best managed conservatively, I am yet to have a client say they regret their decision to pursue CT and surgery for their dog’s tarsal OCD.